
Case Report:
73yo WF presents with 10 day shadow developing in the vision. Found to have superior temporal bullous RRD w multiple pinholes reaching into the fovea. Part of the RD was clear indicating a chronic RD with extension inferiorly with cloudy retina. Severe choroidal atrophied areas temporally. Pt is a habitual eye rubber.
Other Hx: COAG on Xalatan, HTN, elevated cholesterol, vitelliform macular dystrophy.
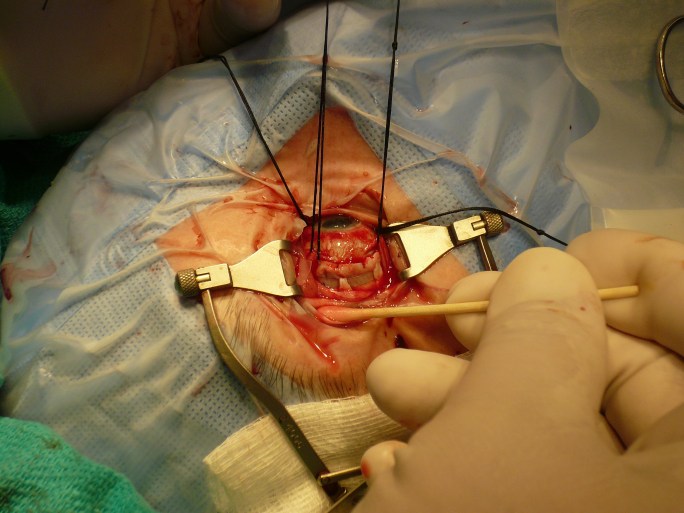
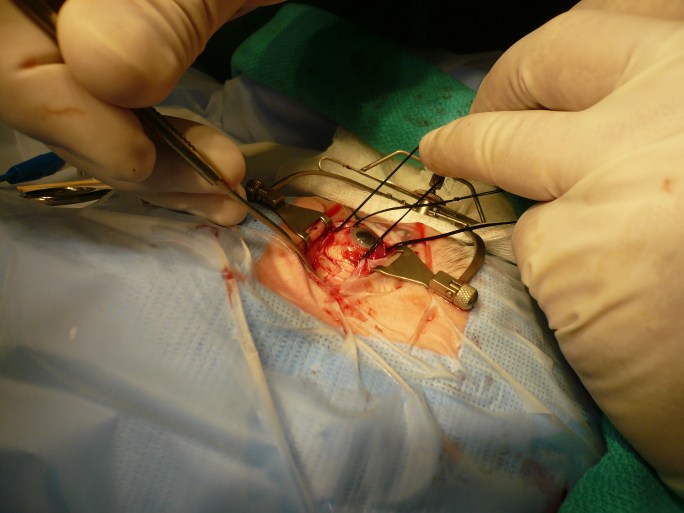
Disposition: SB surgery was started however after the conjunctiva was opened and the cryotherapy with scleral depression was attempted, it was noted that the sclera and choroid was so thin that you could easily see the depressor outside the eye with the binocular indirect from inside view. The sclera was so thin in three quadrants that there was nothing to sew to or make a scleral tunnel. Experience with a family of Sticklers syndrome and their retinal detachments had shown the utility of scleral patch grafting as in their case, a 17 year old buckle had eroded though the sclera and opened the eye needing emergency grafting. This experience with the mother and son showed the utility of scleral patch graft under a buckle to prevent erosion and re attach the retina. The thought was to graft donor sclera to the thinned wall of the eye in such a manner to cover the thinned areas with an overlap so that the graft could be sutured at the anterior and posterior edges of the graft to more normal tissue holding the patch in place. Then the problem was there was no buckling effect to the patch so belt loops were placed to hold a 240 band in the right position to support the retina and the patch would keep the buckle in position. The band was overlapped in the inferior nasal quadrant with a 70 sleeve in the one quadrant with sufficient scleral thickness to allow mersylene sutures.

The retina settled significantly but did not finish flattening. Pneumatic retinopexy was tried with an 85% flattening. An epiretinal membrane was present and contracting further therefore vitrectomy with membrane peel, lensectomy, C3F8 gas was used and flattened the retina. Further return of the epiretinal membrane weeks later caused early traction and Subretinal fluid from Proliferative Vitreo-retinopathy and repeat Vitrectomy flattened the retina again. Ultimately the vision returned to about the 20/200-400 level but had an intact fibrotic anterior capsule (aphakic). Pt was noted to have a significant posterior staphiloma on the OCT images OU. Pt also had a pre-existing vitelliform macular scar that limited the return of vision. She has remained stable for many years now at the 20/70 level.
You never know when you will need to combine techniques to solve a problem.
Clinical update…
Here is a BIO video of the eye many years later. You can see the laser and cryo marks but cannot appreciate the buckling effect as it is a gentle curve. Choroidal thinning in the periphery can be seen on some views. There is a vitelliform dystrophy seen in the macula and the vision has been stable at the 20/60-70 range (now pseudophakic).
PVH.
