
 For those of you with either a short memory or missed the early history, here is a brief review as experienced and remembered by one clinician…
For those of you with either a short memory or missed the early history, here is a brief review as experienced and remembered by one clinician…
In the area of wet Age Related Macular Degeneration (ARMD), we have come a long way in my short 35 year experience including residency and fellowship. Here is where I start to sound very old: In the distant past, we only had the laser to stop subretinal neovascular membranes (SRNVM) as long as they were not subfoveal. The laser was about 50% effective at retaining or recovering vision. The other 50% of eyes would re-occur a new SRNVM and would involve the fovea. Alteratively the heat of the laser would create an atrophic spot that affected the fovea eventually over time. This was still a step forward as before the laser there was nearly a 100% reading vision loss as we had nothing. Then the arguments started about which laser to use as new lasers were multi frequency. Red lasers might be better as theoretically they penetrated into the choroid where melanin pigment would absorb the energy and cause the coagulation of the abnormal vessels. Other colors were used such as Yellow and Green (532nm) as they were absorbed by hemoglobin in the vessels and coagulated from within the abnormal vessel. Other physicans stated that argon laser (producing a full thickness retinal burn) was no different in effect than the special frequencies of the other lasers, “ a laser burn is a laser burn no matter which laser makes it“. Personal preferences dictated the treating physician’s choices.
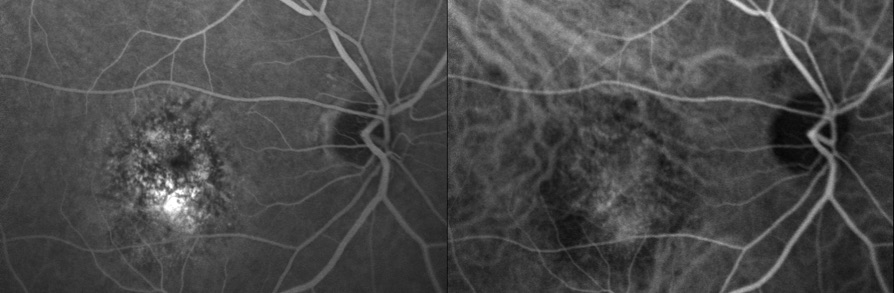
The next series of studies published explored what happend to the subfoveal nets (SRNVM) if not treated. Some found the natural history of very poor outcomes and suggested that sacrificial laser to the fovea may limit the size of the disceform scar that would develop. Many had a problem with the idea to sacrifice the fovea in this case and would not do it. Others decided to do a “Ring laser”, a treatment ring of laser placed just outside the central SRNVM that would try to limit the spread of the foveal SRNVM. This would also limit the elevation of the macula away from the choroid due to the forming the disceform process. In practice, some patients maintained 20/100-200 vision with clearly reduced leakage of the central SRNVM on the fluorescein angiogram after Tx. There were some regaining 20/30-40 vision achieving driving status again. These visions were maintained for many years after treatment. There were a few others that would continue to scar to CF vision dispite all efforts. When Photodynamic therapy was announced, theoretically it should be superior to ring laser and ring laser fell by the wayside.
The announcement of the photodynamic therapy (PDT) system with the low power “cold laser” illuminating the macula to activate the chemotherapeutic drug injected in the vein of the patient seemed to be an answer to every suffering patient with a foveal SRNVM. What was not known until later was that the treatment would increase the production of vascular endothelial growth factor (VEGF) and as a result, there were many reoccurrences of the SRNVM. More treatments of PDT seemed to control the problem up to 5 treatments. At that time any patient that fit the rather limited criteria for treatment was sent to Raleigh to get the treatment rather than the ring laser. Later analysis showed that most of these patients achieved CF vision with a very large atrophic scar centrally about the same size as what would have been the result of no treatment namely a disceform scar with the same vision. This was much poorer that the results of the ring laser. No real advantage to this treatment long term and PDT has mostly fallen out of favor.
Then there was a revolution, the arrival of anti VEGF agents. The first Avastin patient arrived at the clinic with a handful of research papers supporting the use of anti VEGF agents in 2005 and demanding that we should start using it. This individual has multiple degrees especially in engineering and researched the issue to his satisfaction that he tried using DMSO solvent and a protein kinase inhibitor on a small pad placed on the conjunctiva of his eye. This did burn for a little while but seemed to stop the progress as the DMSO solvent would carry the Protein Kinase inhibitor through the conj and sclera. He rather preferred to get Avastin injected than do the PKI-DMSO combination. From time to time he would fail to show up and used the PKI-DMSO to get time between injections lengthened. He was very motivated to find a solution as he had already lost central vision in one eye and did not want to experience this in the other eye.
In the mean time multiple new agents (Lucentis, Eylea, Macugen, Avastin) made the choice of which drug and how often to use them a big challenge. What made this worse for the clinician to make a decision on which to use was all the papers funded by the drug companies proving their results superior to the others made this unbelievable and confusing. The only drug that did not have the reseach funding was Avastin and as such the retina community did reseach showing “non inferiority” of Avastin compared to other drug use. Locally at retina get togethers it was decided to use either 1.25mg or 2.5mg of Avastin on a monthy basis intially. This was decided before any of the other drugs came out.
Now we are in the throws of still figuring out which is the best and how ofter to give them or how to afford these highly expensive drugs (with one exeption). Who knows what is next?
Actually we do have a “what is next” and it is called “Beovu” by it’s commercial name. It has only been out a few months and already there are serious reports of permanent vision loss from Intra Vitreal Inflammation (IVI) that has caused many normal arteries and veins to occlude thought due to a reaction to the drug. Many physicians are not “jumping on the band wagon” on this one as all the other drugs are looking safer and just as effective. It brings to mind the old adage: “Not every thing that is NEW is good!“
PVH
