
The question is which is better double dose of Avastin or Eylea?
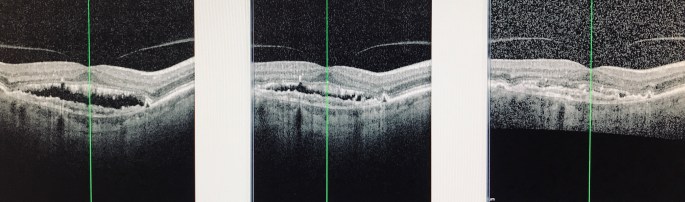
For years I have used double dose Avastin (2.5mg with AC tap for IOP control) to try to control age related macular degeneration. Initially there is a substantial improvement in the subretinal fluid (SRF) and the vision. In certain patients with more longstanding maculopathy, the fluid settles down to a bare minimum and the vision improves to 20/25 as seen in the left image. This may take a while to accomplish. After multiple injections the subretinal fluid does not get any better than this but the vision remains good. We have been taught in the past that this is a treatment failure due to the presence of SRF on OCT. The natural thought process would be try another drug. I would switch to 3 doses of Q4-6 week Eylea treatments but the vision would fall from 20/25 to 20/40 and finally 20/70 in the center and right images above. With declining subretinal fluid it would be reasonable to think that Eylea works better according to the OCT but then what happened to the vision. If this person is put back on Avastin, the subretinal fluid returns back to the level in the left image and the vision improves to 20/25. The patient much prefers this situation and will not go back to Eylea.
I am suspicious that the teaching of the presence of SRF in the macula = treatment failure of a specific drug may be very erroneous. The vision tells more of the story than the OCT does. This example is only one of many patients that are populating the clinic now. These patients tend to be longer standing ARMD patients that possibly have well established subretinal neovascular membranes in the choroid (SRNVM) as seen by the irregularities in the IS/OS junction and RPE layer. If they are more mature, they may not rely on VEGF to maintain their perfusion and the anti VEGF therapy is only preventing new branches from developing. There may be a decreased perfusion of the SRNVM with therapy but it does not go away. Other drugs may have a more profound effect on the retina possibly including the VEGF varieties that control the daily cycles of the rods and cones of the retina thereby affecting the vision function.
These observations and others have made my treatment protocol be double dose Avastin once a month for three months then extend to 6 weeks if stable. A few patients can reach 8 week interval but not much longer. It has been stated that the half life of Avastin in the eye is about 3 weeks for single dose and 6 weeks for double (first order kinetics). It is also interesting to see in the recent papers presented at the 2018 Retina Specialty Day at AAO the observation that Avastin has approximately a 10% effect on the opposite eye. We have seen patients that were early wet ARMD in one eye and more involved other eye. Both improved with injections in the more involved eye only, benefitting both eyes. We have also seen patients with long term (5-10 year course) monocular Avastin therapy that eventually quit therapy on the first eye due to eventual atrophic changes and then a few months later have the second eye turn wet and need therapy. Chronic treatment of one eye actually was protecting the other uninvolved eye. I do not have the numbers just yet as to the size of the opposite eye benefit in Avastin injections but I have not seen this effect with the other drugs. This may reduce the number of total injections needed per patient. Also it allows all the risk of injection to be taken by the “worst eye” while the good one does not need injections.
These are just clinical observations by one clinician on using anti VEGF drugs for 14 years. Sincerely PVH.
